Sunscreen science has evolved far beyond basic UV protection. Today, sunscreens play a core therapeutic role in the management of melasma, pigmentation disorders, and post-procedure skin care.
These recent advancements were discussed in detail during a scientific CME held in Hubli, conducted under the guidance of the Hubli Dharwad Dermatology Society (HDDS), where Dr. Girish Kumar M participated as an invited speaker.
At Ear Science Centre, this year marks a deeply meaningful milestone—10 years of transforming lives through cochlear implant care. What began as a clinical mission has evolved into a movement rooted in hope, inclusion, and equal opportunity for children with hearing loss.
To commemorate this decade-long journey, we brought together our cochlear-implanted children and their families—not as patients, but as confident individuals with stories, voices, and dreams of their own.
A bride’s jewellery is not just an accessory—it’s a symbol of tradition, elegance, and her personal style. Among all the bridal ornaments, the necklace holds a special place as it beautifully enhances the bride’s outfit and overall look. Choosing the right necklace can feel overwhelming, but with the right guidance, you can find the piece that makes you shine on your big day.
ಆಸ್ಪತ್ರೆ ಅಥವಾ ಕ್ಲಿನಿಕ್ ಗಳಲ್ಲಿ ನಾವು ನೋಡುವ ಸಾಮಾನ್ಯ ವಿಷಯವೆಂದರೆ ರೋಗಿಗಳು ರಕ್ತದೊತ್ತಡ (ಬಿಪಿ) ಔಷಧಿಗಳನ್ನು ಪ್ರಾರಂಭಿಸಲು ನಿರಾಕರಿಸುವುದು. ವೈದ್ಯರು "ನಿಮ್ಮ ರಕ್ತದೊತ್ತಡ ಹೆಚ್ಚಾಗಿದೆ" ಎಂದು ಹೇಳಿದಾಗ, ಅನೇಕ ರೋಗಿಗಳು "ನಿನ್ನೆ ರಾತ್ರಿ ನಾನು ಚೆನ್ನಾಗಿ ನಿದ್ರೆ ಮಾಡಲಿಲ್ಲ," "ಕೆಲಸವು ಒತ್ತಡದಿಂದ ಕೂಡಿದೆ," "ಮನೆಯಲ್ಲಿ ಜಗಳವಾಯಿತು," ಅಥವಾ "ನಾನು ಆಸ್ಪತ್ರೆಗೆ ಹೋದಾಗ ನನಗೆ ಭಯವಾಗುತ್ತದೆ" ಅದಕ್ಕೆ ಬಿ.ಪಿ ಜಾಸ್ತಿ ಬಂದಿದೆ ಎಂದು ನೆಪಗಳನ್ನು ನೀಡುತ್ತಾರೆ. ಆದಾಗ್ಯೂ, ನಿಮ್ಮ ರಕ್ತದೊತ್ತಡ ಎರಡು ಪ್ರತ್ಯೇಕ ಸಂದರ್ಭಗಳಲ್ಲಿ, ಕನಿಷ್ಠ 6 ಗಂಟೆಗಳ ಅಂತರದಲ್ಲಿ ಹೆಚ್ಚಿದ್ದರೆ, ನಿಮಗೆ ಅಧಿಕ ರಕ್ತದೊತ್ತಡ ಇರಬಹುದು ಎಂದರ್ಥ.
A 34-year-old female, with giddiness and mild headache for approximately 2 years. She was a mother of two kids, had uneventful pregnancies, and had no other co-morbid diseases. She had consulted for the above complaints for 2 years, and treated by local practitioners, and the ENT evaluations were normal. Multiple physician and neurologist consultations were done.
Men and women, young and old, happiness and sadness - alcohol completes the celebration and occasion. It's not unusual these days to find school and college kids consuming alcohol. Beer, Vodka, Wine, and Whiskey are commonly consumed. Parenting has been much more difficult now a days. Schools and teachers are facing newer challenges with substance abuses.
A 19-year-old, male working as a farmer presented with high-grade fever > 100° F, myalgia, and anemia for 2 months duration. Treated at local hospitals for 6-8 weeks and was referred to us for further management. 15 days later he started developing joint pains involving large and small joints. He did not suffer from any arthritis in the past. No history of fever, sore throat, allergic rashes, bites, or stings in the recent past. He did not have any history of weight loss, cough, hemoptysis, abdomen pain, breathlessness, chest pain, sweating, back pain, urethral discharge, burning urination, or palpitations. No similar complaints in family or contacts. No history of tuberculosis, autoimmune diseases, or recent vaccination.
Examination revealed mild pallor without any lymphadenopathy, splenomegaly, crepts, or ronchi. Initial evaluation revealed he had anemia with hemoglobin of 8.3gm%, WBC count of 20,700 cells/cumm, and PMN of 89%. Peripheral smear was microcytic and hypochromic, neutrophilic leukocytosis with pencil-shaped cells. His creatinine was 0.8mg/dL, however, ultrasonography showed bulky kidneys with raised echotexture. Urine routine examination, Urine for AFB and microscopy were normal. Serum albumin was 2.7g/dL - s/o malnutrition vs acute phase reactant. The Widal test was positive at 1: 160. Brucella and Rheumatoid factor were negative. Malaria Rapid and QBC smear were negative. A blood culture was sent.
He was started on broad-spectrum antibiotics along with atypical coverage. Day 5 was completed, fever was recurring. Over the next couple of days, he developed left knee joint swelling, associated with effusion. ROM was restricted along with local redness. USG-guided effusion was tapped and sent for analysis. Effusion was turbid with 200 cells, predominantly neutrophils, and few lymphoid cells. Fluid biochemistry was s/o acute inflammatory exudate. The synovial fluid culture was negative. Blood culture was negative on day 7.
The fever was persistent. Further workup was done towards ANA Profile, Vasculitis panel, and Echocardiogram for infective endocarditis showed no vegetation. GeneXpert MTB on Urine, Synovial fluid, and Sputum were negative. Fundoscopy showed no evidence of choroid tubercles and uveitis. CECT Thorax, abdomen, and pelvis with oral and IV contrast were unremarkable.
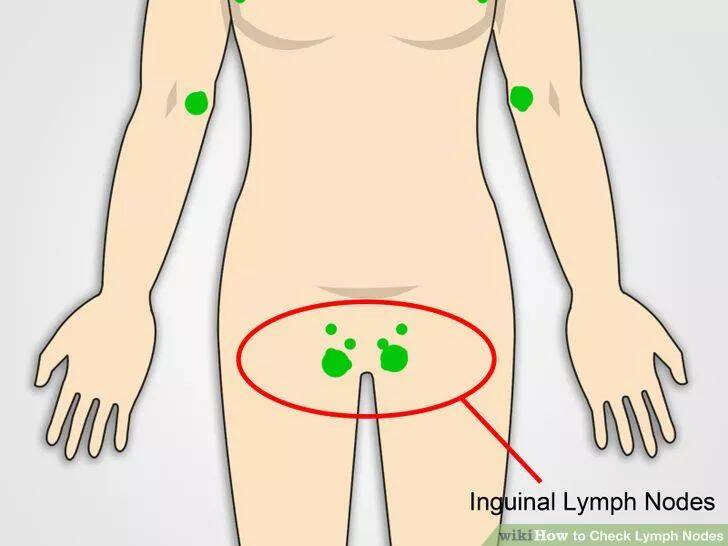
4 weeks passed by, fever was recurrent and persistent. In 5th week patient developed Right Inguinal Lymphadenopathy. FNAC was reported to be reactive lymphadenitis. Excision biopsy of the same was negative for TB, Granulomas, and Malignancy. VDRL was negative, and CSF analysis was also normal.
As all workup was negative, IGRA was planned. However, due to economic constraints, the patient was unwilling for the test. Finally, Poncet's was considered a diagnosis of exclusion, and anti-tubercular medications were started. Weight band adjusted ATT (anti-tubercular therapy under NTEP regimen) was started. The patient felt significant improvement in general health, febrile episodes were absent by 48 hours. Appetite improved. CRP showed a decreasing trend.
Blood was transfused in view of anemia. Iron supplements and multivitamins were started. After 4 days of afebrile episodes, the patient was discharged with a diagnosis of Poncet's disease.
Poncet's disease is an unusual manifestation of active or latent tuberculosis manifesting as reactive arthritis. It's usually a diagnosis of exclusion. In developing countries like India, Tuberculosis poses immense challenges to physicians because of its myriad presentations.
Case Highlight: Dr. Chetan K Ganteppanavar, Director and Consultant Physician at Kalpana Multi Speciality Clinic, Hubli, managed a challenging case of Poncet's disease. The patient, a young farmer, presented with persistent fever and joint pain. Extensive investigations ruled out other conditions, and despite negative TB tests, Poncet's disease was diagnosed based on clinical judgment. The patient responded remarkably well to ATT, highlighting the importance of considering TB in differential diagnoses, especially in endemic areas.
Conclusion:Poncet's disease, though rare, should be considered in patients with unexplained polyarthritis, particularly in TB-endemic regions. Early diagnosis and prompt ATT can lead to complete recovery, underscoring the critical role of clinical acumen in managing such complex cases.
In today's fast-paced world, unhealthy lifestyles have become the norm. Lack of exercise, frequent dining at hotels and restaurants, stressful jobs, and disrupted sleep patterns contribute significantly to lifestyle-related diseases. Among these, hypertension or high blood pressure (BP) is emerging as a major concern, even among individuals as young as 18 to 20 years. Decades ago, doctors rarely checked BP in young adults, but today, no age group can be ignored. I, Dr. Chetan K Ganteppanavar, Consultant Physician in Hubli, share my clinical experiences with young hypertensive patients, emphasizing the need for early detection and management.
Case Studies on Hypertension in Young Adults
Patient 1: A 22-Year-Old Medical Student with Severe Hypertension
A 22-year-old medical student casually asked his colleague to check his BP, only to discover a shocking reading of 200/100 mmHg. This was confirmed using a different machine. He was tall and overweight, with a stressful work schedule, poor dietary habits, and no regular exercise. Family history revealed diabetes, hypertension, and premature cardiac atherosclerotic diseases. Despite extensive blood tests and imaging, no secondary cause was identified. A strict low-salt diet, weight loss regimen, and regular exercise were recommended. With adherence to these lifestyle modifications, along with Telmisartan, Cilnidipine, and Minoxidil, his BP was brought under control.
Patient 2: A 20-Year-Old MBBS Student Diagnosed with Primary Hypertension
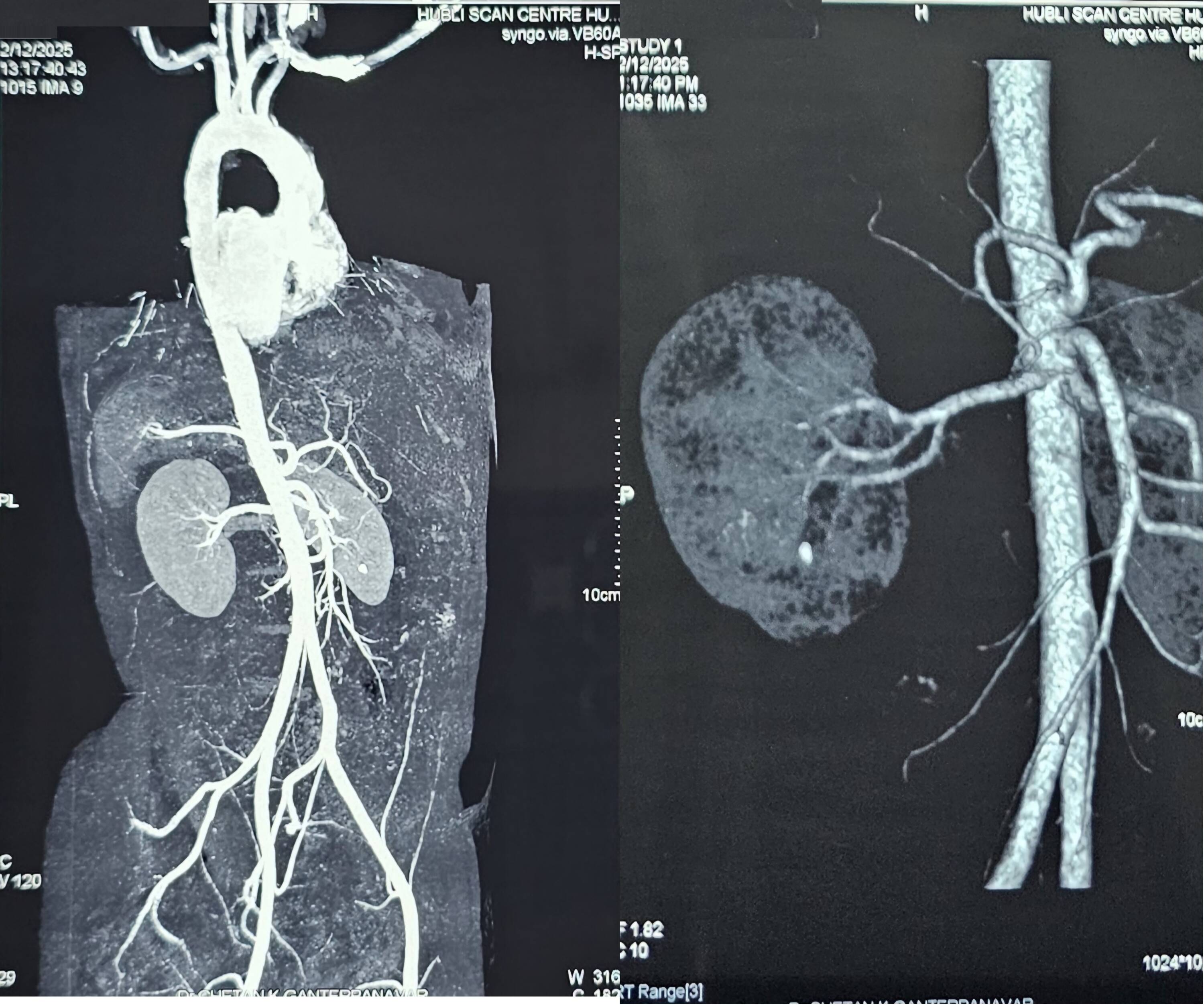
A 20-year-old MBBS student admitted for Rickettsial fever was found to have a BP of 180/110 mmHg. A significant family history of hypertension was noted. His diet was predominantly non-vegetarian, and he frequently ate at the hostel or restaurants. Although physically active in sports twice a week, his BP remained elevated. Extensive investigations, including CT abdomen with aortogram and renal artery angiogram, ruled out secondary causes. He was diagnosed with primary hypertension and treated with Telmisartan, Cilnidipine, and Chlorthalidone.
Patient 3: A 24-Year-Old MD Aspirant with Anxiety and Hypertension
A 24-year-old preparing for MD exams presented with anger outbursts, palpitations, insomnia, and anxiety, exacerbated by tea and coffee. On examination, he had short stature, Grade I obesity, acanthosis nigricans, and a BP of 150/100 mmHg. His family history was significant for diabetes and hypertension. Work-up for secondary hypertension was negative. Diagnosed with primary hypertension, he was started on Metoprolol and Telmisartan, which controlled both his BP and anxiety symptoms.
Patient 4: A 23-Year-Old MBBS Student with Recurrent Headaches
A 23-year-old final-year MBBS student presented with recurrent headaches and was found to have BP >160/90 mmHg. He was obese, had poor dietary habits, and led a sedentary lifestyle. Unlike the other cases, there was no significant family history. A thorough evaluation ruled out secondary causes such as hypokalemic hypertension, pheochromocytoma, and carotid body tumors. Diagnosed with primary hypertension, he was successfully managed with Telmisartan and Cilnidipine.
Hypertension in Young Adults : A Growing Concern
The cases above highlight a worrying trend—hypertension among young medical professionals, a demographic that constitutes less than 0.05% of the general population. If such high numbers are seen among doctors, the prevalence in the general population could be significantly greater.
Young individuals diagnosed with hypertension require extensive evaluation to rule out secondary causes like hyperthyroidism, pituitary tumors, renal artery stenosis, coarctation of the aorta, pheochromocytoma, and renin-angiotensin abnormalities.
Managing Hypertension needs a Multi-Faceted approach:
First-line agents like Calcium Channel Blockers (CCBs), Beta-Blockers, Angiotensin-Converting Enzyme Inhibitors (ACEi), Angiotensin Receptor Blockers (ARBs), and Diuretics. The cornerstones of management are: Low salt diet avoiding processed foods, regular physical activity – 150 minutes/week along with yoga, meditation, and good sleep, early detection through regular health check-ups, avoiding caffeine, alcohol, and tobacco, and adequate hydration.
Potential Complications of Uncontrolled Hypertension :
Increased risk of heart attack, left ventricular hypertrophy, and heart failure, chronic kidney disease, dialysis dependency, hemorrhagic or ischemic strokes, retinopathy leading to vision problems, gangrene , peripheral vascular disease and dementia.
Conclusion :
Hypertension in young adults is no longer a rarity. The modern lifestyle, characterized by stress, poor diet, and lack of exercise, is fueling its rise. Early screening, comprehensive evaluation, and timely intervention are crucial in preventing long-term complications such as cardiovascular diseases, kidney failure, and stroke. As healthcare professionals, we must lead by example, adopting healthier lifestyles and promoting awareness among the general population.
For those looking for the best doctor in Hubli for hypertension management, expert consultation, and comprehensive care, I, Dr. Chetan K Ganteppanavar, an experienced physician in Hubli, am dedicated to providing personalized and evidence-based treatment approaches for my patients.
Dr. Chetan K Ganteppanavar Physician & Diabetologist, Hubli, Karnataka, India
Tags : Hypertension, Young High BP, BP in teenage, Complications high BP,